
There’s a scene in the popular medical drama House in which the show’s namesake is seen scrawling on his left leg with a black permanent marker, “NOT THIS LEG.” He’s due for an operation on his right leg, and as a doctor himself, he’s all too aware that mistakes are made during surgery; he doesn’t want the surgeon operating on the wrong leg.
This may seem overly cautious and farfetched, but a 2016 study in the medical journal The BMJ found that medical errors, if classified as a disease, would be the third-leading cause of death in the United States behind cancer and heart disease.
To compound what many say is a fractured medical system, it’s a recognized fact that rural healthcare in America is up against many challenges. Rural communities face physician shortages and people are often forced to travel long distances. More travel and greater numbers of medical providers increases the likelihood of confused or lost medical records.
Patient misidentification is a leading cause of medical malpractice and skyrocketing medical costs, identified by the Joint Commission of the United States and the World Health Organization. In fact, it is estimated that 33 cents of every dollar in the medical sector is spent on administrative tasks like registration and correcting errors in health records.
Guy Hembroff ’98 ’16, associate professor in the College of Computing and director of the health informatics graduate program, aims to change that.
“Any type of data exchange between medical providers relies on identifying the patient correctly,” Hembroff says, noting that one of the biggest issues is that an individual may end up with multiple record files because of a slight name misspelling.

Health informatics graduate students demo mixed reality patient and health records review.
It’s Hembroff’s goal to improve patient care and outcomes, particularly in rural areas. To achieve this goal, Hembroff is designing a phased approach that integrates patient care and addresses gaps in care. Using specially developed algorithms, artificial intelligence (AI), wearable sensors, computer vision (training computers to understand our visual world), and image analysis (enhancing or extracting useful information from images), he’s rewriting how rural healthcare is administered to help individuals and communities.
Under the Umbrella
Hembroff’s phased approach includes the development of a global identification algorithm: Unique Medical Biometric Recognition and Enforcement of Legitimate and Large-scale Authentication (UMBRELLA). The algorithm uses touchless biometric identification—fingerprints and secondary biometric verification, such as facial recognition, by using cameras on standard devices like smart phones and laptops—rather than passwords for both patient and provider, which makes medical data more secure. The creation of a unique health identifier ensures that patient records are seamlessly integrated, rather than scattered, and potentially duplicated, between various providers.
“UMBRELLA provides secure identification and authorization for individuals, and feeds into personal health libraries,” Hembroff says. “Its architecture provides a solution to integrate a patient’s currently siloed digital health data—physical, behavioral, personal—to help ensure a holistic and accurate view of the individual’s health, while empowering patients to better self-manage their health.”
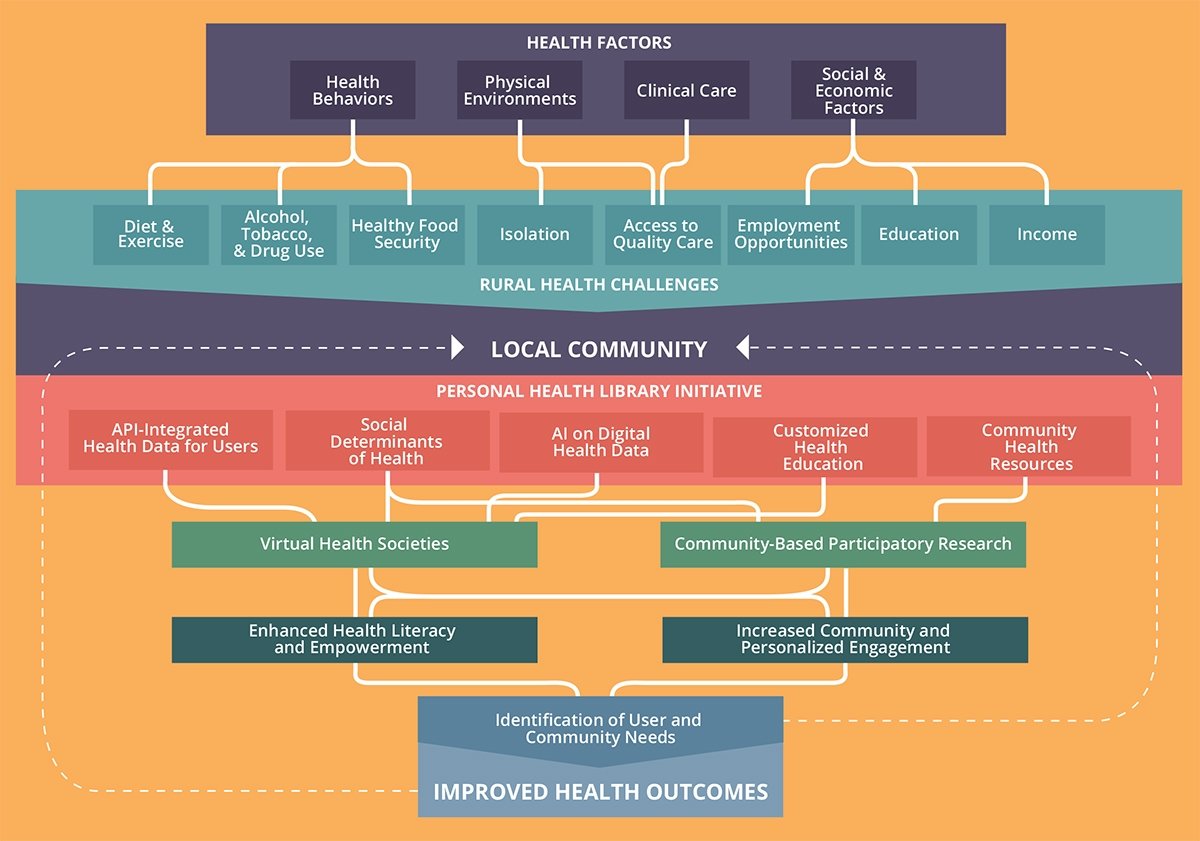
Hembroff’s model integrates partnerships and addresses gaps to overcome rural healthcare challenges.
Hembroff’s system puts patients in control of their own health records, and gives patients the power to determine what information they wish to share. In a world where insurance companies, social media companies, and even online shopping portals gather users’ personal data, Hembroff’s app is a step toward better medical privacy, more understandable interfaces without complicated medical coding, and individual control.
Plus, the approach ensures doctors have all of the information they need to treat a patient—a powerful commodity in a health system where the average amount of time clinical doctors spend consulting with patients is only a few minutes.
Community Care
The second phase of Hembroff’s work empowers communities to improve health outcomes by integrating information into community health and safety planning.
Health is more than the results from an annual physical. Health factors include health behaviors, physical environment, social and economic factors, and clinical care. Our medical system focuses on clinical care largely, relegating other factors as less important. However, an individual’s environment and social and economic indicators are “social determinants of health,” which are responsible for 50 percent of health outcomes, while clinical care is responsible for just 20 percent.
As an example, if a person can’t get in to see a dentist, by the time the person does eventually receive dental care, the care is likely to focus on extracting rotted teeth, rather than on preventative care. Hembroff’s integrated model feeds medical information (stripped of personal identifiers) to local health organizations, so communities can collectively improve the social determinants of health. For example, many communities around the country have chosen to fluoridate their water supplies to improve dental health. Another option is to reduce the amount of sugary foods or treats available in schools.
Hembroff is working on algorithms to customize health education and community resources to residents. He gives the example of a person living in a remote part of the Upper Peninsula, working two jobs with weight-related health issues; it could be a daunting task to locate, purchase, and prepare healthy food for their family. Through the person’s digital personal health library, preventative education and community-coordinated incentives can be tailored to help find nearby locations to purchase healthy food, explain how to make the healthy meals on a budget, and describe the benefits of doing so. Hembroff’s model links users to these resources in the app. But the app can also be used by public programs—police, shelters, food banks—to allocate resources more strategically to community members who need them, wasting less money and creating a culture of community health and safety as a priority. One community space in particular has a lot of potential.

"There's a big role communities can play in the health of their residents. Chronic diseases don't occur in isolation, but rather are closely affiliated to an individual's culture, behavior, and environment."
Nearly 95 percent of Americans live near public libraries, and Hembroff wants to see public libraries become repositories of accessible and reliable health information. Not everyone has access to technology, but libraries are a widely trusted public resource and a place where residents will often go to research different health concerns.
In coordination with community health organizations, libraries are in the position to offer adequate technology access and assistance to those in need. Hembroff hopes community health care professionals could begin holding office hours of sorts at libraries to educate people—a sort of in-person WebMD.
The applicability of Hembroff’s work isn’t limited to communities bounded by geographic location; his model creates virtual health societies that help people get healthier by interacting with peers. Social isolation, lack of physicians, and inaccessible specialty services are more likely in rural communities than in urban. Virtual health communities are being tested using natural language processing algorithms to identify patterns of user questions and provide validated responses aimed at improving the education and health of those who utilize it.
Going the Distance
Phase three, which Hembroff will work on next, integrates secure telemedicine and remote monitoring with AI, to help create a proactive care management approach while addressing gaps in rural healthcare.
Algorithm-assisted medical data scanning can alert providers to potential issues, like potentially harmful drug interactions, risk stratification, disease progression modeling, and precision medicine. Coupled with advanced monitoring applications, such data can shorten the distances between providers and patients to make more frequent visits—the virtual kind—easier and more impactful.
“While there are many challenges associated with rural healthcare delivery, there is a dedicated passion from medical practitioners to improve care delivery and the expense of healthcare in their community,” Hembroff says. “If technology is done right, it can help support this passion by overcoming many of the barriers of rural healthcare.”
Michigan Technological University is an R1 public research university founded in 1885 in Houghton, and is home to nearly 7,500 students from more than 60 countries around the world. Consistently ranked among the best universities in the country for return on investment, Michigan's flagship technological university offers more than 185 undergraduate and graduate degree programs in science, technology, engineering, mathematics, computing, forestry, business, health professions, robotics, psychology, social sciences, humanities, and the arts. The rural campus is situated just miles from Lake Superior in Michigan's Upper Peninsula, offering year-round opportunities for outdoor adventure.



